
Dysphagia – Symptoms, Causes, and Treatment Options
Dysphagia is the medical term for difficulty swallowing, a condition that can affect eating, drinking, and overall quality of life. People with dysphagia often describe the sensation of food “sticking” in the throat or chest, coughing or choking while eating, or pain when swallowing.
Many people with dysphagia find support and improved swallowing with physiotherapy for dysphagia, where specialized exercises help strengthen muscles and restore safe swallowing patterns. Nutrition for dysphagia provides tailored dietary guidance to make eating easier, more comfortable, and nourishing. Acupuncture for dysphagia may also help by relaxing tension, improving circulation, and supporting the nervous system to enhance swallowing function. Together, these services create a holistic approach to managing dysphagia and improving quality of life.
Overview of Dysphagia
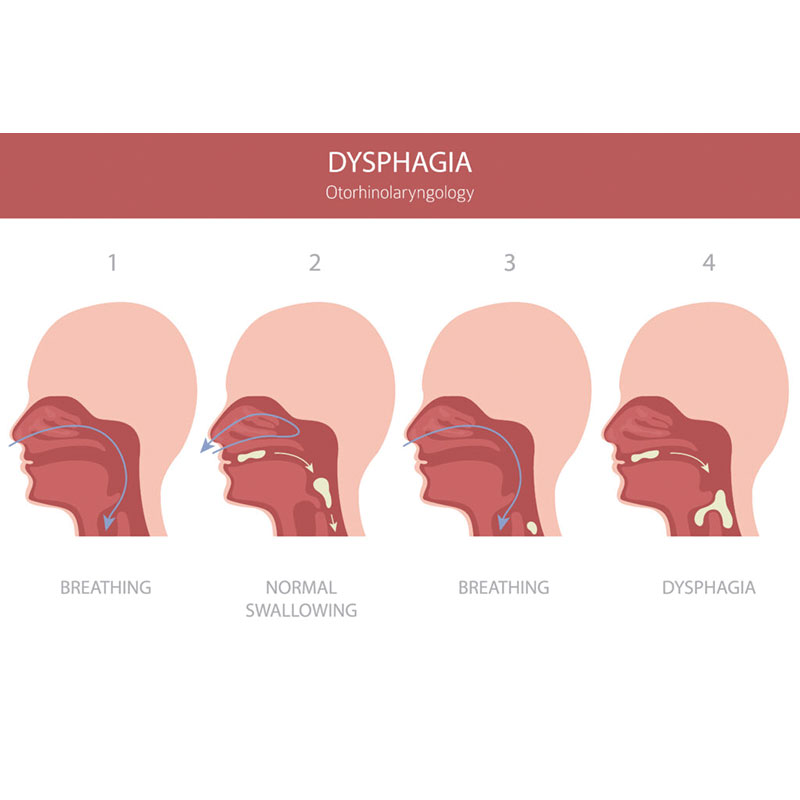
Dysphagia means you have trouble swallowing food, liquid, or sometimes even saliva. It can happen because of problems with the muscles and nerves that control swallowing or due to structural issues in the throat or esophagus. Dysphagia is not a disease itself, but a symptom of many underlying conditions, ranging from minor throat irritation to serious neurological or gastrointestinal disorders.
How common is dysphagia?
Dysphagia is more common than many people realize. Studies suggest that up to 13% of adults may experience swallowing difficulties at some point, and prevalence rises sharply with age. In older adults living in care facilities, the rate may be as high as 50–60% depending on health conditions. Dysphagia is also frequently seen in people recovering from stroke, those with Parkinson’s disease, multiple sclerosis, or head and neck cancers.
Daily life impact of dysphagia
The impact of dysphagia goes well beyond mealtimes:
- Work and productivity: Difficulty eating can make social or professional meals stressful, leading some people to avoid them.
- Sports and activity: If hydration is difficult, it may affect endurance and performance.
- Sleep: Nighttime choking episodes or reflux-related swallowing difficulties can disturb rest.
- Relationships: Shared meals may become anxiety-provoking, reducing social interaction.
- Mental health: Chronic dysphagia is linked to stress, embarrassment, and even depression due to the fear of choking or malnutrition.
Compared with simple sore throat or indigestion, dysphagia tends to persist, worsen, or come with other concerning symptoms such as unexplained weight loss or frequent chest infections.
Symptoms of Dysphagia
The main symptom of dysphagia is difficulty swallowing, but the way it feels can vary from person to person. Some experience only mild discomfort, while others face severe challenges that affect nutrition and safety.
What are the main symptoms of dysphagia?
- Food sticking: Feeling like food is caught in your throat or chest.
- Coughing or choking: Especially when eating or drinking thin liquids.
- Pain when swallowing (odynophagia): A burning or stabbing sensation.
- Drooling or difficulty managing saliva.
- Unintentional weight loss: From avoiding food or poor nutrition.
- Frequent respiratory infections: Caused by food or liquid entering the airway (aspiration).
How severe can dysphagia get?
- Mild dysphagia: May cause occasional coughing or slow eating.
- Moderate dysphagia: Leads to avoidance of certain textures, longer mealtimes, or anxiety about eating.
- Severe dysphagia: Can result in malnutrition, dehydration, and medical emergencies like aspiration pneumonia.
How does dysphagia affect daily life?
- Work: You may feel self-conscious eating with colleagues.
- Sport and exercise: Risk of dehydration if drinking is difficult.
- Sleep: Choking at night or reflux-related issues may wake you.
- Relationships and mood: Many people report social isolation, frustration, and lowered confidence.
Red flag signs of dysphagia
See a healthcare provider right away if you notice:
- Sudden or rapidly worsening swallowing problems.
- Difficulty swallowing both liquids and solids.
- Unexplained weight loss or persistent chest pain.
- Frequent pneumonia or chest infections.
Reference:
Baijens LWJ, et al. (2016). European Society for Swallowing Disorders – European Union Geriatric Medicine Society white paper: oropharyngeal dysphagia as a geriatric syndrome. Clinical Interventions in Aging, 11: 1403–1428. doi:10.2147/CIA.S107750
Causes and Risk Factors for Dysphagia
Dysphagia can be caused by structural blockages, muscle or nerve problems, or systemic health conditions. The exact cause depends on where the swallowing process breaks down—mouth, throat, or esophagus.
Common causes of dysphagia
- Neurological conditions: Stroke, Parkinson’s disease, multiple sclerosis, or ALS can disrupt nerve control of swallowing.
- Muscle disorders: Conditions like myasthenia gravis or muscular dystrophy weaken swallowing muscles.
- Obstructions: Narrowing of the esophagus (strictures), tumors, or growths can physically block food passage.
- Reflux disease (GERD): Acid reflux may scar or narrow the esophagus.
- Infections or inflammation: Chronic irritation can cause swelling and difficulty swallowing.
Lifestyle and risk factors
- Age: Swallowing muscles weaken naturally with age, making dysphagia more common in seniors.
- Posture: Poor posture, especially in those with mobility issues, may worsen swallowing function.
- Occupation: People exposed to chronic irritants (e.g., dust, chemicals) may develop throat or esophageal changes.
- Obesity or pregnancy: Can worsen reflux, increasing risk of swallowing problems.
- Cancer treatment: Surgery or radiation for head and neck cancers often affects swallowing.
How is dysphagia different from other swallowing issues?
- Compared with globus sensation (lump in throat): Dysphagia involves real difficulty moving food, not just a feeling.
- Compared with indigestion or reflux: Dysphagia focuses on swallowing function, not just stomach discomfort.
Why identifying risk factors matters
Understanding the cause helps target treatment—neurological dysphagia requires rehabilitation and exercise, while obstructive causes may need surgical or endoscopic intervention.
Diagnosis, Recovery, and Management of Dysphagia
Dysphagia, or difficulty swallowing, requires careful evaluation and tailored management to ensure safety, restore function, and prevent long-term complications. This section explains how dysphagia is diagnosed, what recovery typically looks like, and evidence-based ways it can be managed in daily life.
Diagnosis of Dysphagia
Dysphagia is diagnosed through a combination of history-taking, physical exam, functional tests, and sometimes imaging studies. Because it can result from neurological, muscular, or structural issues, diagnosis focuses on identifying both the swallowing difficulty and its underlying cause.
How do doctors test for dysphagia?
Your doctor will usually start with a clinical interview and a physical exam. They’ll ask when the swallowing problems began, whether you struggle more with solids or liquids, and if you’ve experienced choking, coughing, or weight loss. They may observe you swallowing different textures to see where the difficulty occurs.
Common diagnostic tools include:
- Bedside swallowing assessment: A speech-language pathologist watches you swallow food and liquids, noting signs of coughing, throat clearing, or “wet” voice quality.
- Videofluoroscopic swallow study (VFSS): A moving X-ray taken while you swallow contrast-coated food to show where the process breaks down.
- Fiberoptic endoscopic evaluation of swallowing (FEES): A flexible scope is inserted through the nose to view the throat while you swallow.
- Esophageal manometry: Measures muscle contractions in the esophagus to detect motility problems.
- Upper endoscopy (EGD): Used to rule out tumors, strictures, or inflammation.
How do clinicians identify the root cause of dysphagia?
The goal is to distinguish between:
- Oropharyngeal dysphagia – difficulty starting a swallow, often due to neurological or muscular problems.
- Esophageal dysphagia – food sticking lower in the chest, often due to narrowing, reflux damage, or motility disorders.
By clarifying the type of dysphagia, doctors can choose the most effective treatment. For example, stroke-related dysphagia may respond to targeted rehabilitation, while reflux-related dysphagia may need medication and lifestyle changes.
How is dysphagia different from other swallowing complaints?
- Globus sensation feels like a lump in the throat but does not usually affect actual swallowing.
- GERD (acid reflux) can mimic dysphagia but primarily causes heartburn and regurgitation.
- Dry mouth (xerostomia) may make swallowing uncomfortable but is not true dysphagia.
Reference:
Logemann JA. (1998). Evaluation and Treatment of Swallowing Disorders. 2nd ed. Pro-Ed.
Recovery Timeline for Dysphagia
Recovery from dysphagia varies widely depending on its cause, severity, and the timeliness of treatment. Some people recover quickly, while others may require long-term rehabilitation and lifestyle adjustments.
How long does dysphagia usually take to improve?
- Mild dysphagia: Often improves within a few weeks to months with swallowing exercises, dietary adjustments, and posture training.
- Moderate dysphagia: May require 3–6 months of therapy and consistent support from speech-language pathologists.
- Severe dysphagia: Recovery may take 6–12 months or longer, especially when caused by progressive neurological diseases or following cancer treatment.
What factors affect recovery?
- Cause of dysphagia: Stroke-related dysphagia often improves, while conditions like Parkinson’s may require ongoing management.
- Age: Older adults may recover more slowly due to weaker muscles and multiple health issues.
- Nutrition and hydration: Poor intake can slow healing.
- Consistency of therapy: Regular swallowing exercises lead to better outcomes.
Decision pathway (if/then logic)
- If your dysphagia is mild (occasional choking, no weight loss), then dietary changes and posture techniques may be enough.
- If your dysphagia is moderate (frequent coughing, meal avoidance), then structured swallowing therapy and possibly temporary texture-modified diets are recommended.
- If your dysphagia is severe (weight loss, aspiration pneumonia), then you may need a feeding tube initially while undergoing intensive rehabilitation.
Return to daily life with dysphagia
- Work: Many people return to professional activities but may need meal adaptations (soft diet, longer breaks).
- Sport and activity: Safe hydration strategies are key; endurance athletes may need thicker fluids.
- Relationships: Shared meals are possible with planning and support; therapy often restores confidence.
- Long-term: With the right strategies, most people adapt well and maintain independence.
Reference:
Martino R, et al. (2005). Dysphagia after stroke: incidence, diagnosis, and pulmonary complications. Stroke, 36(12): 2756–2763. doi:10.1161/01.STR.0000190056.76543.eb
How to Manage Dysphagia
Management of dysphagia focuses on making swallowing safer, improving nutrition, and restoring as much function as possible. Treatment plans are tailored to the cause and severity.
What’s the best way to manage dysphagia at home?
Self-help & relief tips (step-by-step)
- Adjust your posture: Sit upright while eating and remain upright for at least 30 minutes afterward.
- Take small bites and sips: Give your muscles time to work.
- Modify food textures: Soft, moist foods are easier to swallow than dry or crumbly foods.
- Try thickened liquids: These move more slowly, reducing the risk of choking.
- Focus on mealtime: Eliminate distractions and eat slowly.
These strategies can reduce risks while you undergo formal treatment.
Therapy and professional interventions
- Speech-language pathology therapy: The cornerstone of dysphagia management. Exercises strengthen muscles, improve coordination, and train safer swallowing patterns.
- Dietary modifications: Dietitians design texture-modified diets to maintain adequate calories and hydration.
- Medical treatments: Proton pump inhibitors for reflux, dilation for strictures, or surgery for tumors may be required.
- Feeding tubes: For severe or high-risk cases, temporary or permanent enteral feeding ensures nutrition while therapy continues.
Lifestyle and long-term prevention strategies
- Ergonomics: Proper head and neck alignment improves swallowing safety.
- Strength and flexibility: Regular swallowing exercises help maintain progress.
- Stress management: Anxiety can worsen symptoms; mindfulness or counseling may help.
- Community support: Dysphagia support groups provide encouragement and shared coping strategies.
How is managing dysphagia different from other conditions?
Unlike reflux or indigestion, dysphagia management focuses on airway safety and preventing aspiration, making therapy more specialized and multidisciplinary.
Multidisciplinary Coordinated Care for Dysphagia at CARESPACE
CARESPACE treats dysphagia with a coordinated, team-based approach that addresses not only the physical challenges of swallowing but also the psychological, nutritional, and lifestyle factors that affect recovery. Instead of seeing one provider at a time, you benefit from a circle of care that communicates and collaborates to help you regain function, confidence, and quality of life.
How does CARESPACE treat dysphagia differently?
Most clinics approach dysphagia from a single perspective, but CARESPACE integrates multiple disciplines into one coordinated plan. This ensures you receive comprehensive care for both the swallowing problem and the issues that often come with it—such as nutrition, posture, stress, and overall health.
A typical journey might look like this:
- You begin with a physiotherapy assessment to evaluate posture, neck mobility, and muscle coordination that may influence swallowing.
- You are referred to a dietitian to ensure you’re still getting adequate calories and hydration, even if you need a modified diet.
- At the same time, a psychotherapist may support you in coping with the anxiety or embarrassment that often comes with eating difficulties.
- If muscle tension contributes to discomfort, massage therapy or acupuncture may be added for relaxation and improved blood flow.
This collaboration allows you to progress faster and avoid the gaps that happen when care is fragmented.
Why does a team approach help dysphagia recovery faster?
Dysphagia is rarely caused by one problem alone. It may stem from neurological issues, structural changes, muscle weakness, or lifestyle factors. Treating only one angle often leaves people struggling. CARESPACE’s team-based approach ensures all these pieces are addressed together.
- Physiotherapy and chiropractic care improve neck and spine alignment, which can ease swallowing mechanics.
- Massage therapy and acupuncture reduce tightness in surrounding muscles that may worsen discomfort.
- Nutrition and naturopathic medicine ensure your body has the energy and resources to heal, while adapting meals to your abilities.
- Psychotherapy and mental performance coaching reduce the fear of choking, help with social confidence, and support sleep if anxiety is keeping you awake.
- Kinesiology and fitness training restore overall strength and endurance, helping you maintain independence and prevent secondary issues like deconditioning.
Together, these services not only treat the swallowing difficulty but also support your whole health—physical, emotional, and social.
What does coordinated dysphagia care at CARESPACE look like in practice?
CARESPACE organizes your care into phases: acute, subacute, and maintenance. Each step is tailored to your current needs and adjusted as you recover.
- Acute phase (immediate support): Focus on safety and symptom relief. Nutrition counseling ensures safe food textures, while physiotherapy may recommend swallowing techniques. If stress is high, psychotherapy or coaching helps you cope.
- Subacute phase (restoring function): You gradually strengthen the muscles involved in swallowing with guided exercises, while massage therapy or acupuncture helps with relaxation. Ergonomic adjustments and postural work support more natural swallowing.
- Maintenance phase (long-term wellness): Once symptoms improve, the team shifts to prevention. Dietitians help you maintain a balanced diet, fitness coaches keep you active, and ongoing psychotherapy ensures you feel confident in social and mealtime situations.
For example, if you are recovering from a stroke, your plan may include speech therapy exercises (through your hospital team) combined with CARESPACE physiotherapy, nutrition support, and counseling. This holistic structure helps you avoid complications like malnutrition or social withdrawal.
How does CARESPACE support mental health with dysphagia?
Living with dysphagia is not just a physical challenge—it affects your confidence, relationships, and emotional health. CARESPACE includes mental health professionals as part of your care plan so you never feel isolated in your recovery.
- Psychotherapy provides coping tools for meal anxiety, embarrassment, or depression.
- Mental performance coaching helps you build resilience and adapt socially, so you can enjoy meals again without fear.
- Nutrition and naturopathic medicine support better sleep and energy levels, which can be disrupted by stress or poor intake.
- Exercise and kinesiology improve mood and reduce overall anxiety through safe, structured activity.
This integrated approach ensures you recover both physically and emotionally, reducing the long-term toll dysphagia can take.
Why choose multidisciplinary coordinated care instead of single-discipline care?
The unique advantage of CARESPACE is its ability to bring all these providers together under one roof. Instead of trying one treatment at a time, you benefit from a shared plan where providers communicate, update each other, and adjust your care as you progress.
Benefits include:
- Faster recovery: Multiple factors—muscle strength, posture, nutrition, stress—are treated at once.
- Lower recurrence risk: Long-term habits like posture correction, balanced diet, and coping strategies are built into your plan.
- Personalized care: Every program is adapted to your lifestyle, whether you are a working professional, athlete, or senior.
- Peace of mind: You know your providers are working as a team, not separately.
While single-discipline care might offer short-term relief, coordinated multidisciplinary care sets you up for sustainable recovery and improved quality of life.
Related Conditions, FAQs, and Disclaimer for Dysphagia
Dysphagia (difficulty swallowing) can overlap with or mimic several other health conditions, which makes accurate diagnosis and care especially important. This section explores related conditions, answers the most common client questions, and provides compliance information to ensure clarity and trust.
Related Conditions for Dysphagia
Several conditions can present with symptoms similar to dysphagia, or may increase your risk of developing swallowing difficulties. Understanding these related conditions helps ensure you receive the right evaluation and treatment.
- Gastroesophageal reflux disease (GERD): Acid reflux can cause inflammation and narrowing of the esophagus, making swallowing more difficult.
- Stroke and neurological disorders: Conditions like Parkinson’s disease, ALS, or multiple sclerosis often impair the nerves and muscles needed for safe
- swallowing.
- Head and neck cancers: Tumors or cancer treatments (radiation, surgery) can change the structure of the throat and esophagus.
- Esophageal strictures or achalasia: Narrowing or motility problems in the esophagus may mimic dysphagia.
- Globus sensation: A feeling of a lump in the throat that isn’t related to actual food passage difficulty.
Because dysphagia can be confused with these other problems, professional assessment is essential to pinpoint the cause.
Explore our full Conditions List to learn more about related swallowing and digestive conditions.
Looking for information on a different condition? Visit our full Conditions List.
FAQs About Dysphagia
The fastest relief usually comes from adjusting food textures and eating posture. Soft or pureed foods and sitting upright while eating reduce choking risk and discomfort. Thickened liquids can also make swallowing safer.
In the short term, avoiding dry, sticky, or crumbly foods can ease symptoms. Longer-term relief depends on the underlying cause—whether that’s reflux, neurological changes, or esophageal narrowing. A speech-language pathologist can recommend safe strategies tailored to your needs.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have dysphagia, consult a qualified health provider.
Mild dysphagia may improve on its own, especially if it’s caused by a temporary throat infection or irritation. Drinking plenty of fluids and resting the throat often helps.
However, persistent or worsening dysphagia usually does not resolve without treatment. If caused by neurological issues, strictures, or reflux, you’ll likely need therapy, medical treatment, or dietary adjustments. Early intervention prevents complications like aspiration pneumonia or malnutrition.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have dysphagia, consult a qualified health provider.
You should see a doctor if swallowing problems last more than a few days, are getting worse, or interfere with nutrition. Red flag signs include unexplained weight loss, chest pain, frequent choking, or repeated chest infections.
A doctor can run tests such as swallow studies, endoscopy, or manometry to find the root cause. Even if your case feels mild, early evaluation ensures you get the right support before complications develop.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have dysphagia, consult a qualified health provider.
Swallowing therapy exercises strengthen the muscles involved in swallowing and improve coordination. These may include:
- Effortful swallow: Swallowing hard to activate more muscles.
- Mendelsohn maneuver: Holding the throat in a higher position during a swallow.
- Masako maneuver: Swallowing while gently holding the tongue forward.
These exercises are usually guided by a speech-language pathologist. Attempting them without guidance may not be effective and could increase risks. Exercises are most helpful when customized to your swallowing pattern.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have dysphagia, consult a qualified health provider.
Posture makes a big difference with dysphagia. Sitting upright (or standing) during meals usually makes swallowing safer and easier. Reclining or lying down increases the risk of choking or aspiration.
If you notice that symptoms change with position, it’s important to share this with your healthcare provider. They may recommend specific postures, such as chin tuck or head turn, to make swallowing more effective.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have dysphagia, consult a qualified health provider.
No, surgery is not always required. Most people improve with non-surgical care, such as swallowing therapy, dietary adjustments, and medications for reflux.
Surgery is considered only if there is a physical blockage, such as an esophageal stricture, tumor, or achalasia that does not respond to other treatments. Even then, less invasive procedures like dilation may be tried before surgery.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have dysphagia, consult a qualified health provider.
Prevention depends on the cause of dysphagia. For reflux-related swallowing problems, lifestyle changes such as avoiding late meals, elevating the head of the bed, and limiting acidic foods help. For neurological conditions, ongoing therapy and exercises can maintain swallowing strength.
Good oral hygiene, eating slowly, and staying upright after meals also reduce recurrence. Working with a multidisciplinary team—speech therapy, nutrition, and medical providers—provides the best long-term protection.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have dysphagia, consult a qualified health provider.
Shape
Dysphagia is difficulty moving food or liquid from the mouth to the stomach, while reflux and indigestion involve discomfort after food reaches the stomach.
Dysphagia: food “sticks” in the throat or chest, coughing, choking, weight loss risk.
Reflux: heartburn, sour taste, regurgitation, sometimes leading to esophageal narrowing that can cause dysphagia later.
Recognizing the difference is important because dysphagia may indicate more serious conditions requiring direct evaluation.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have dysphagia, consult a qualified health provider.
Articles on Dysphagia
For more information, you can view all dysphagia articles on our resource hub.
Authorship & Disclaimer
Reviewed by: Mahnoor Naveed, Acupuncturist
Last Updated: September 7th, 2025
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have dysphagia, consult a qualified health provider.