
Achalasia – Symptoms, Causes, and Treatment Options
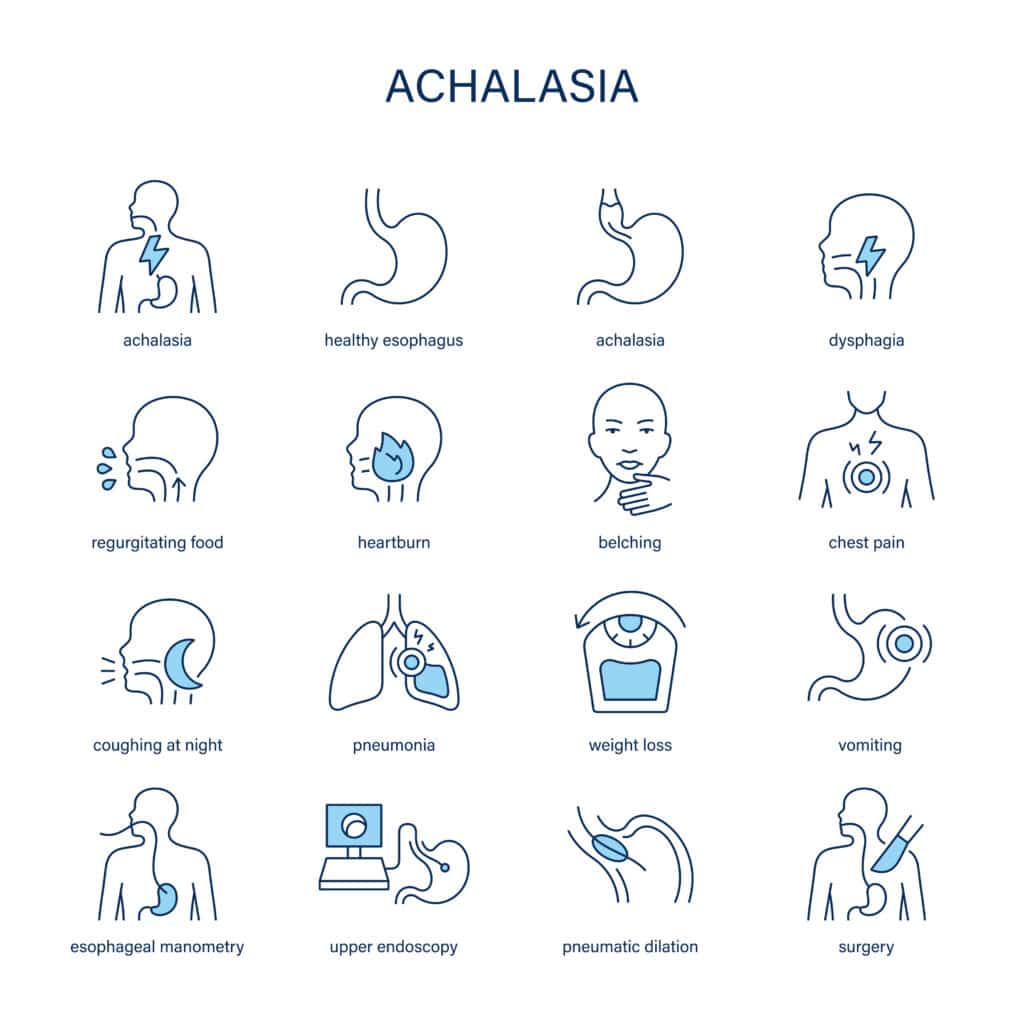
Achalasia is a rare condition that affects the esophagus—the tube that carries food from your mouth to your stomach. It happens when the lower esophageal sphincter (LES), a muscular valve at the bottom of the esophagus, does not relax properly. As a result, food and liquids have trouble passing into the stomach. The most common symptoms are difficulty swallowing, chest pain, regurgitation of food, and unintentional weight loss.
Many people with achalasia find support and symptom relief with physiotherapy for achalasia, where breathing and postural exercises can improve chest mobility and ease swallowing-related tension. Massage for achalasia may help reduce muscle tightness in the chest and upper back, promoting relaxation and comfort. Chiropractic care for achalasia can support spinal alignment, improving nerve function and reducing pressure that may contribute to discomfort. Our kinesiologist-guided achalasia rehab can also provide gentle movement strategies to enhance overall strength, posture, and resilience. Together, these services create a supportive approach to help you feel more at ease and improve your quality of life.
Overview of Achalasia
Achalasia is a chronic disorder of the esophagus that makes swallowing difficult. It occurs because the nerves controlling the muscles of the esophagus become damaged, leading to weak or uncoordinated contractions. This means the esophagus cannot move food downward efficiently, and the LES remains tight instead of opening.
How common is Achalasia?
Achalasia is considered rare, affecting about 1 in every 100,000 people each year worldwide. While it can occur at any age, it is most often diagnosed between the ages of 25 and 60. Men and women are affected at similar rates. Because the symptoms can be vague and progress slowly, many people may go undiagnosed for years.
Impact of Achalasia on daily life
Living with Achalasia can affect many aspects of your daily routine:
- Eating and drinking: Meals may take much longer, as food feels “stuck.” Many people avoid eating in social settings out of fear of choking or coughing.
- Work and productivity: Ongoing fatigue from poor nutrition or disrupted sleep can affect concentration and job performance.
- Sports and physical activity: Lack of proper nutrition can lead to weakness, reduced stamina, and slower recovery from exercise.
- Sleep: Regurgitation of food, especially when lying down, can cause disturbed sleep and even increase the risk of aspiration (food entering the airway).
- Mental health and relationships: Social embarrassment, fear of choking, and weight changes can contribute to anxiety, depression, or withdrawal from social life.
How is Achalasia different from acid reflux?
People sometimes confuse Achalasia with gastroesophageal reflux disease (GERD) because both conditions cause regurgitation and chest discomfort. However, in GERD, the LES is too loose, letting acid flow back into the esophagus. In Achalasia, the LES is too tight and fails to relax, preventing food from passing into the stomach.
Reference: Vaezi, M.F., Pandolfino, J.E., Vela, M.F. (2017). ACG Clinical Guidelines: Diagnosis and Management of Achalasia. American Journal of Gastroenterology, 112(3), 429–442. https://doi.org/10.1038/ajg.2016.556
Symptoms of Achalasia
The hallmark symptom of Achalasia is trouble swallowing (dysphagia) for both solids and liquids. Unlike other swallowing disorders that affect only solid food, Achalasia causes difficulty with nearly everything swallowed.
What are the main symptoms of Achalasia?
- Difficulty swallowing (dysphagia): Feels like food is stuck in the chest. This is often worse with bread, meat, or dry food.
- Regurgitation: Food or liquid coming back up, sometimes hours after eating. This can lead to coughing, bad breath, or aspiration into the lungs.
- Chest pain or discomfort: A squeezing or burning sensation that can mimic heart problems. Pain may occur during meals or at rest.
- Weight loss: Often gradual, due to reduced intake and poor absorption of nutrition.
- Heartburn-like symptoms: Some people report burning in the chest, but unlike GERD, it is due to trapped food rather than stomach acid.
Functional and lifestyle impact
- Work and daily tasks: Frequent interruptions to eat slowly, or the need to avoid certain foods, can reduce productivity.
- Sleep disruption: Nighttime regurgitation may wake you up coughing or choking.
- Sports and physical activity: Reduced nutrition may cause fatigue, weakness, or muscle loss.
- Emotional health: Constant worry about choking in public or avoiding meals with friends can lead to stress and isolation.
When should you see a doctor?
Seek medical care if you experience:
- Persistent trouble swallowing both solids and liquids.
- Unexplained weight loss over weeks or months.
- Chest pain that mimics heart problems.
- Recurring nighttime coughing or choking.
Causes and Risk Factors for Achalasia
Achalasia develops when the nerves of the esophagus degenerate, leading to poor muscle function and a non-relaxing LES. The exact cause is unknown, but research points to both biological and lifestyle factors.
What causes Achalasia?
- Nerve damage (neurological dysfunction): The loss of nerve cells that control esophageal muscles is the main driver.
- Autoimmune factors: The body’s immune system may mistakenly attack nerve cells in the esophagus.
- Viral or infectious triggers: Past infections may play a role in some people.
- Genetic predisposition: While rare, families with multiple cases suggest a possible genetic influence.
Risk factors and lifestyle influences
While anyone can develop Achalasia, certain factors may increase the risk:
- Age: Most often diagnosed between 25 and 60 years.
- Pregnancy: Can worsen swallowing difficulties due to pressure on the stomach and esophagus.
- Body weight: Both obesity (pressure on the stomach) and extreme weight loss (weakened muscles) can complicate symptoms.
- Occupation and posture: Jobs requiring frequent bending or heavy lifting may worsen regurgitation and chest discomfort.
- Other health conditions: Conditions like autoimmune disease or prior esophageal surgery may contribute.
How is Achalasia different from similar conditions?
- GERD vs. Achalasia: In GERD, food flows backward; in Achalasia, it cannot flow forward.
- Esophageal cancer vs. Achalasia: Both can cause swallowing trouble, but cancer typically progresses faster and may involve pain localized to one area.
- Diffuse esophageal spasm vs. Achalasia: Spasm involves abnormal muscle contractions, while Achalasia involves absent peristalsis and a tight LES.
Daily life impact of risk factors
- Nutrition challenges: Restricted diets and fear of eating may lead to malnutrition.
- Mental health strain: Living with a chronic swallowing disorder can increase stress, anxiety, or depression.
- Relationships: Shared meals become difficult, often leading to avoidance of social situations.
Diagnosis, Recovery, and Management of Achalasia
Achalasia is a rare but serious disorder of the esophagus that requires a structured clinical pathway. Getting the right diagnosis early, understanding what recovery might look like, and learning effective management strategies are key to improving quality of life. Below, we’ll walk through how Achalasia is diagnosed, what to expect in terms of recovery and prognosis, and how to manage symptoms long term.
Diagnosis of Achalasia
Achalasia is diagnosed through a combination of clinical evaluation, functional tests, and imaging studies. Because its symptoms can mimic other conditions such as acid reflux or esophageal cancer, accurate testing is essential.
How do doctors test for Achalasia?
Doctors usually start with a medical history and physical exam, followed by specialized tests:
- Clinical interview and physical exam
- Your doctor will ask about swallowing problems, regurgitation, chest pain, and weight loss.
- They may look for signs of malnutrition or complications like lung issues from aspiration.
- Esophageal manometry (gold standard test)
- This test measures how well the esophagus contracts and whether the LES relaxes properly.
- In Achalasia, manometry shows absent peristalsis (no wave-like motion) and a tight LES that does not relax.
- Barium swallow (X-ray with contrast)
- You drink a chalky liquid that coats the esophagus. X-rays then show whether food is stuck or if the esophagus looks dilated.
- The classic sign of Achalasia is a “bird’s beak” appearance at the LES, where the lower esophagus narrows sharply.
- Endoscopy (esophagogastroduodenoscopy or EGD)
- A thin scope is passed into the esophagus to rule out cancer, strictures, or other conditions.
- While endoscopy may look normal in early Achalasia, it is essential to exclude malignancy.
How do doctors confirm it’s Achalasia and not something else?
Doctors rule out other disorders that look similar:
- GERD (acid reflux): Symptoms overlap, but reflux shows a weak sphincter, not a tight one.
- Esophageal cancer: Both cause swallowing difficulty, but cancer usually progresses faster and can be seen on endoscopy.
- Esophageal spasm: Spasms cause pain and swallowing issues, but manometry patterns are different.
Identifying the root cause
Doctors focus on whether Achalasia is primary (nerve degeneration with no known cause) or secondary (due to another condition such as cancer or prior infection). Identifying the root cause ensures the right treatment pathway is chosen.
Reference: Edoardo Vincenzo Savarino, Renato Salvador, Matteo Ghisa, Amir Mari, Francesca Forattini, Andrea Costantini, Roberto De Giorgio, Giovanni Zaninotto, Research gap in esophageal achalasia: a narrative review, Diseases of the Esophagus, Volume 37, Issue 8, August 2024, doae024, https://doi.org/10.1093/dote/doae024
Recovery and Prognosis for Achalasia
Recovery from Achalasia depends on the severity of symptoms, treatment approach, and individual health factors. While Achalasia cannot be completely “cured,” treatments can relieve symptoms and help people return to normal life.
How long does recovery from Achalasia take?
- Mild cases (early diagnosis):
- After treatments like pneumatic dilation or medication, relief may occur within weeks.
- Many return to work and regular meals within 1–2 months.
- Moderate cases:
- Patients who undergo surgery (Heller myotomy or POEM) may take several weeks to recover, with gradual improvement in swallowing.
- A soft diet is usually recommended for the first few weeks.
- Severe cases (long-standing Achalasia):
- In people with a very dilated esophagus or major weight loss, recovery may take months.
- Some may require ongoing monitoring, repeat procedures, or dietary modifications.
What is the long-term outlook for Achalasia?
- Relapse and recurrence: Symptoms may come back in 15–30% of patients, often years after initial treatment.
- Risk of complications: Long-term untreated Achalasia may increase the risk of aspiration pneumonia and esophageal cancer.
- Factors influencing outcomes: Age, type of treatment, severity at diagnosis, and adherence to follow-up care all affect prognosis.
Decision pathway: if/then logic
- If Achalasia is diagnosed early → then minimally invasive treatments (dilation, medications) may provide long-term relief.
- If Achalasia is moderate or progressing → then surgery (Heller myotomy or POEM) is often recommended for lasting results.
- If Achalasia is severe or complicated → then treatment may require a combination of surgery, nutrition support, and close monitoring.
Returning to daily life
- Work: Most people can return to work within weeks after treatment, though fatigue may linger if nutrition was poor before treatment.
- Sports: Light activity may resume within 2–4 weeks, with full sports participation after doctor clearance.
- Lifestyle: Many patients report improved quality of life, reduced fear of eating, and better sleep once regurgitation is controlled.
Reference: Oude Nijhuis, R.A.B., Zaninotto, G., Roman, S., et al. (2020). European Guidelines on Achalasia: United European Gastroenterology and European Society of Neurogastroenterology and Motility recommendations. United European Gastroenterology Journal, 8(1), 13–33. https://doi.org/10.1177/2050640620903213
Management of Achalasia
Managing Achalasia involves a mix of medical treatment, lifestyle adjustments, and long-term follow-up. Even after procedures, self-care strategies can reduce symptoms and improve well-being.
What’s the best way to manage Achalasia at home?
Doctors may recommend combining medical therapies with practical lifestyle strategies:
- Posture and eating habits
- Eat slowly, chew thoroughly, and drink water between bites.
- Stay upright after meals for at least 1–2 hours to prevent regurgitation.
- Elevate the head of your bed to reduce nighttime symptoms.
- Activity modification
- Avoid vigorous exercise immediately after meals.
- Use relaxation techniques to manage stress, which can worsen symptoms.
- Diet adjustments
- Choose softer foods (soups, yogurt, smoothies) during flare-ups.
- Avoid very dry or sticky foods like bread and peanut butter.
- Small, frequent meals are often easier to tolerate than large meals.
Step-by-step self-help & relief tips
- Sit upright during and after meals.
- Take small bites and chew thoroughly.
- Sip warm water to help relax the esophagus.
- Eat soft foods when symptoms worsen.
- Sleep with your head elevated to reduce nighttime regurgitation.
These steps don’t cure Achalasia, but they can make daily life much easier.
Therapy and long-term management approaches
- Medical procedures: Pneumatic dilation, Heller myotomy, or POEM can provide long-lasting relief.
- Medications: Nitrates or calcium channel blockers may be used for people who cannot undergo procedures, though effects are temporary.
- Therapy and coaching: Nutrition counseling, habit coaching, and sometimes psychological support can help patients adapt to lifestyle changes.
- Community and social support: Joining support groups can help reduce isolation and provide encouragement.
Preventing long-term complications
- Regular follow-up with a gastroenterologist is essential to monitor for recurrence.
- Ongoing surveillance may include repeat manometry, endoscopy, or imaging if symptoms reappear.
Reference: Vaezi, M.F., Pandolfino, J.E., Yadlapati, R.H., et al. (2020). ACG Clinical Guidelines: Diagnosis and Management of Achalasia. American Journal of Gastroenterology, 115(9), 1393–1411. https://doi.org/10.14309/ajg.0000000000000731
Multidisciplinary Coordinated Care for Achalasia at CARESPACE
At CARESPACE, we believe that treating Achalasia requires more than just addressing the physical swallowing problem. Because this condition affects your eating, sleeping, emotional health, and overall lifestyle, our approach combines multiple disciplines into one coordinated care plan. This ensures you get comprehensive support for both the physical and psychological impacts of Achalasia.
How does CARESPACE treat Achalasia differently?
CARESPACE takes a team-based, multidisciplinary approach to Achalasia, integrating physical therapies, mental health care, and lifestyle coaching. Unlike standard care that often relies only on surgery or medication, we support you with natural, evidence-based therapies that help reduce symptoms, improve recovery, and prevent recurrence.
- Chiropractic and Physiotherapy: Focus on posture, breathing mechanics, and thoracic mobility to reduce chest pressure and support swallowing.
- Massage Therapy and Kinesiology: Help ease upper body tension, improve relaxation, and enhance muscle function for daily comfort.
- Psychotherapy and Mental Performance Coaching: Address stress, anxiety, and social avoidance that often come with Achalasia.
- Nutrition and Naturopathic Medicine: Support safe, comfortable eating with customized diet strategies, meal modifications, and supplements when appropriate.
- Acupuncture and Relaxation Therapy: Assist with stress reduction and symptom relief, especially in cases of chest discomfort and insomnia.
Why does a team approach help Achalasia recover faster?
A coordinated team reduces recovery time by targeting Achalasia from multiple angles at once. When disciplines work together, you get a care plan that covers both immediate symptom relief and long-term prevention.
Acute phase (new diagnosis or worsening symptoms)
- A physiotherapist may focus on breathing strategies and posture correction to ease swallowing.
- A massage therapist helps reduce chest wall tension from repeated swallowing strain.
- A psychotherapist provides tools for managing anxiety and stress related to eating.
Subacute phase (after initial treatment or procedure)
- A nutritionist designs a safe diet plan with soft foods and gradual reintroduction of more complex meals.
- A kinesiologist or fitness trainer develops gentle exercise routines to restore energy and reduce fatigue.
- Acupuncture may be integrated to promote relaxation and improve digestive function.
Maintenance phase (long-term care and prevention)
- Chiropractic care supports spinal mobility, reducing postural stress on the esophagus and chest.
- Mental performance coaching helps you build confidence with eating in social settings.
- Ongoing team check-ins ensure your plan adapts as your symptoms or lifestyle change.
This phased approach ensures you don’t just “get through” the condition—you build resilience for the long term.
How does CARESPACE support the mental health side of Achalasia?
Achalasia doesn’t just affect your body—it impacts your emotional health, relationships, and confidence. At CARESPACE, we integrate psychotherapy, coaching, and lifestyle strategies so you feel supported beyond the physical symptoms.
- Psychotherapy: Helps you manage stress, anxiety about choking, and social withdrawal.
- Cognitive-behavioral strategies: Teach you how to reduce negative thought patterns around eating.
- Nutrition support: Ensures you get adequate nourishment, which directly affects mood and energy.
- Exercise therapy: Boosts endorphins, reduces stress, and helps maintain healthy weight despite dietary challenges.
- Sleep coaching: Addresses insomnia caused by regurgitation or anxiety, restoring better rest cycles.
- By combining these supports, you not only reduce symptoms but also build confidence and resilience in daily life.
The CARESPACE advantage: coordinated care vs. single-discipline care
Standard care often addresses only one part of Achalasia, while CARESPACE brings multiple experts together under one plan.
- Single-discipline approach: A surgeon may treat the tight esophageal sphincter, but you’re left without support for nutrition, posture, stress, or lifestyle changes.
- Multidisciplinary approach: At CARESPACE, your physiotherapist, chiropractor, nutritionist, massage therapist, and psychotherapist share notes, coordinate goals, and build a plan designed for you.
Benefits of coordinated care at CARESPACE
- Faster recovery: Multiple supports working in parallel shorten timelines.
- Lower recurrence risk: Ongoing posture, nutrition, and stress management reduce flare-ups.
- Personalized strategies: Care adapts to your lifestyle, work demands, and emotional needs.
- Whole-person healing: You get support for both physical swallowing issues and psychological impacts like anxiety and insomnia.
Putting it all together: a sample care journey
Imagine you’re newly diagnosed with Achalasia. You may begin with a physiotherapy assessment to learn posture strategies for swallowing. At the same time, a nutritionist helps you adapt meals to prevent food sticking. You’re also referred to massage therapy for chest tension and psychotherapy for eating-related anxiety.
As you progress, you add exercise therapy to rebuild strength and endurance, and coaching to restore confidence in social dining. Over time, this coordinated pathway not only manages Achalasia but helps you return to work, enjoy meals with family, and regain restful sleep.
Related Conditions, FAQs, and Disclaimer for Achalasia
Achalasia often overlaps with or mimics other digestive and swallowing disorders, which can make diagnosis and treatment confusing. Understanding related conditions, frequently asked questions, and clear medical disclaimers helps you feel informed and supported as you navigate care.
Related Conditions for Achalasia
Achalasia shares symptoms with several other conditions, making it important to rule them out through testing.
- Gastroesophageal Reflux Disease (GERD): Unlike Achalasia, GERD occurs when the lower esophageal sphincter is too loose, allowing acid to flow backward into the esophagus.
- Esophageal Cancer: Both conditions cause trouble swallowing, but cancer usually progresses faster and may show structural changes on endoscopy.
- Esophageal Stricture: Narrowing of the esophagus from scar tissue, often due to long-term acid reflux, can mimic Achalasia but has a different underlying cause.
- Esophageal Spasm: Abnormal, strong contractions of the esophagus cause chest pain and swallowing issues but show a different pattern on manometry.
- Diffuse Motility Disorders: Other rare nerve or muscle disorders of the esophagus can appear similar but require different treatment approaches.
Looking for information on a different condition? Visit our full Conditions List.
FAQs About Achalasia
If you’re dealing with Achalasia, you may have questions about symptoms, causes, and the best treatment options available. Below, we’ve outlined the most important information to help you understand Achalasia, what recovery might look like, and how CARESPACE can support you with a personalized care plan.
The fastest relief for Achalasia usually comes from medical procedures like pneumatic dilation or surgery, but short-term comfort can also be found with posture and diet strategies. For example, sitting upright while eating, chewing food very thoroughly, and drinking warm water can make swallowing easier. Some people find avoiding very dry or tough foods helps reduce discomfort.
However, these strategies only manage symptoms temporarily. Long-term relief often requires medical intervention, such as a Heller myotomy (surgery to relax the esophageal sphincter) or POEM (peroral endoscopic myotomy). If you are experiencing persistent swallowing difficulties, you should see a gastroenterologist.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have Achalasia, consult a qualified health provider.
No, Achalasia does not resolve on its own. The condition is caused by nerve damage in the esophagus, which does not naturally repair itself. While symptoms may fluctuate, the swallowing problem usually worsens over time without treatment.
Some people adapt by changing their eating habits—such as switching to softer foods or taking smaller bites—but this does not stop disease progression. Left untreated, Achalasia can lead to severe weight loss, malnutrition, and an increased risk of aspiration pneumonia.
The good news is that effective treatments exist, from balloon dilation to surgical and minimally invasive procedures. These treatments provide long-term relief and improve quality of life.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have Achalasia, consult a qualified health provider.
You should see a doctor if you have persistent difficulty swallowing both solids and liquids, unexplained weight loss, or frequent regurgitation of food. Chest pain, frequent coughing at night, or repeated episodes of choking are also red flag symptoms.
Many people delay care because they assume swallowing problems are due to acid reflux. But unlike reflux, Achalasia does not improve with over-the-counter antacids. Early diagnosis allows for more effective treatment and prevents complications such as aspiration pneumonia or malnutrition.
If symptoms persist for more than a few weeks, or if they interfere with your daily life, schedule a medical evaluation with a gastroenterologist.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have Achalasia, consult a qualified health provider.
Exercises cannot cure Achalasia, but they can improve posture, breathing, and relaxation, which may ease some symptoms. The focus is on reducing chest tension and supporting better swallowing mechanics.
Helpful strategies include:
- Postural exercises: Sitting or standing tall during meals helps food pass more easily.
- Breathing exercises: Slow diaphragmatic breathing may reduce esophageal pressure.
- Gentle stretching: Neck and upper chest stretches help relax tight muscles involved in swallowing.
These strategies are best combined with medical care. They may not prevent food from sticking, but they can reduce discomfort and anxiety around eating.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have Achalasia, consult a qualified health provider.
Yes, your body position can affect Achalasia symptoms. Lying flat after eating often makes regurgitation and nighttime coughing worse. Standing or sitting upright helps food move downward more easily.
Sleeping with your head elevated on a wedge pillow or raising the head of your bed can also reduce nighttime symptoms. This position uses gravity to prevent food and liquid from pooling in the esophagus.
While posture can help manage symptoms, it does not address the underlying nerve problem. It should be used alongside medical treatments recommended by your doctor.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have Achalasia, consult a qualified health provider.
No, not all Achalasia cases require surgery, but most benefit from some form of medical procedure. Treatment options include:
- Pneumatic dilation: A balloon stretches the LES to allow food to pass.
- Botulinum toxin injections: Temporary relief for those who cannot undergo surgery.
- Surgical options (Heller myotomy or POEM): Long-term solutions for many patients.
Mild cases may be managed temporarily with medication, but these are usually less effective. Ultimately, most people require a procedure to achieve lasting relief.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have Achalasia, consult a qualified health provider.
Achalasia cannot be fully prevented, but recurrence of symptoms can often be managed with follow-up care and lifestyle strategies. Even after successful surgery or dilation, some patients experience return of swallowing problems years later.
Prevention strategies include:
- Attending regular follow-up visits with your gastroenterologist.
- Maintaining good posture during and after meals.
- Eating smaller, softer meals to reduce strain.
- Managing stress, which can make swallowing symptoms feel worse.
Ongoing monitoring helps detect problems early, allowing for timely intervention before symptoms worsen.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have Achalasia, consult a qualified health provider.
Yes, it is very common to feel stress, embarrassment, or isolation when living with Achalasia. Eating is a deeply social activity, and difficulty swallowing can make people avoid restaurants, family meals, or even dating.
It is also normal to feel anxious about choking or frustrated by dietary restrictions. These emotional impacts are a valid part of the condition and should not be ignored. Supportive care through counseling, nutrition therapy, and social support groups can make a big difference in emotional well-being.
If you are struggling emotionally with Achalasia, seeking support is an important step in managing the condition.
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have Achalasia, consult a qualified health provider.
Articles on Achalasia

For more information, you can view all achalasia articles on our resource hub.
Authorship & Disclaimer
Reviewed by: Ellen Layton, Nurse Practitioner
Last Updated: September 13th, 2025
Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. If you think you may have an achalasia, consult a qualified health provider.